Be yourself; Everyone else is already taken.
— Oscar Wilde.
This is the first post on my new blog. I’m just getting this new blog going, so stay tuned for more. Subscribe below to get notified when I post new updates.
Be yourself; Everyone else is already taken.
— Oscar Wilde.
This is the first post on my new blog. I’m just getting this new blog going, so stay tuned for more. Subscribe below to get notified when I post new updates.

The World Health Organization (WHO) underscored the quintessential role of quality health care by highlighting that the Sustainable Development Goals (SDGs) are a reaffirmation of the global commitment to attain universal health coverage by the year 2030 and this implies that “all people and communities, everywhere in the world, should have access to the high-quality health services they need – promotive, preventive, curative, rehabilitative, or palliative – without facing financial hardship” (WHO, 2018, p.7). In spite of the emphasis on the quality of health to any nation, it is a paradox that the United States of America (USA) spends more on health than other high-income countries but it has a lower life expectancy, higher infant mortality rate, and worse health.
According to the Commonwealth Health Fund report, “the analysis shows that in the U.S., which spent an average of $9,086 per person annually, life expectancy was 78.8 years
Switzerland, the second-highest-spending country, spent $6,325 per person and had a life expectancy of 82.9 years [but] mortality rates for cancer were among the lowest in the US…” (Commonwealth Fund, 2019, p.3). The major driving force in fuelling the underachievement of the USA healthcare system in terms of money spent per capita and failure to achieve the population outcomes of nations that spend much less per capita on healthcare is the wrong incentives that are in place, America’s revenue maximization philosophy that manifests in exorbitant costs and salaries, inequalities that impinge on social determinants of health, as well as lack of a universal health care insurance.
In terms of its expenditure on health care, in 2016, the USA spent 17.8 percent of its gross domestic product (GDP) on healthcare at a time other nations spent as low as 9.6 percent of GDP (Australia) to a high of 12.4 percent of GDP for Switzerland (Rapaport, 2018, p.1). In addition, the United States of America spent an average of $1,443 per person on drugs as compared to an average of $749 per person in other countries (ibid) yet its life expectancy was the lowest at 78.8 years compared to other countries whose life expectancy ranged from 80.7 years to 83.9 years (Rapaport, 2018, p.1). The USA topped the list of countries studied with regards to child mortality rates at 5.8 fatalities out of every 1,000 live births compared to 3.6 fatalities for every 1,000 live births in other countries (ibid). This clearly demonstrates the USA’s quality of health care is poorer than other wealthy nations due to a myriad of reasons as explained below. In the words of the World Health Organization (2018);
“High-quality health services involve the right care, at the right time, responding
to the service users’ needs and preferences, while minimizing harm and resource
waste. Quality health care increases the likelihood of desired health outcomes and
is consistent with seven measurable characteristics: effectiveness, safety, people centeredness, timeliness, equity, integration of care and efficiency” (WHO, 2018, p.6).
The major reason for the high expenditures in the health care system is the “lack of a universal health care insurance and the demand for more treatments, medicine, and procedures” (Johnson, 2018). As a result, prices for services and procedures are higher in the United States of America as compared to other developed nations as illustrated in Table 1 below.

Table 1: USA healthcare prices
Schuster, McGlynn and Brook’s (2005)research to fathom how good the quality of health care is in the United States showed that there are large gaps between the care people should receive and the care they receive in preventive, acute, and chronic care for all age groups, types of health care facilities and for different types of health insurance.
In the United States of America, high health costs have been cited as a major contributor to bankruptcy and most people are uninsured and bear the brunt of high deductibles and copayments (Hall, 2014). The high costs of health insurance in the country are, therefore, one of the causes of high expenditure on health that is not commensurate with the quality of healthcare for the USA.
The USA healthcare system is characterized by exorbitant administrative costs that are higher than Canada and other countries and the expenditures as well as the “higher prices for medical services and pharmaceuticals and much higher pay for physicians and nurse” (Meyer, 2018, p.1) were cited in the JAMA study in 2016 as the major factors behind USA’s spending a larger share of GDP on healthcare in 2016 than 10 other developed nations (ibid). The major factors were highlighted as excessive utilization of the USA fee-for-service payment system, defensive medicine due to liability worries, failure to invest in social programs, as well as a poor mix of primary care to specialty care (Meyer, 2018, p.1).
The high administrative costs in the USA, which constituted eight percent of healthcare spending in 2016, are partly due to the payment systems in place which are characterized by hundreds of private and public payers who have their own rates with service providers and drug manufacturers and this contrasts with other developed nations where a single public health plan or private insurers are in place which “pay the same nationally negotiated prices” (Meyer, 2018, p.4). It is apparent that administrative costs are a major stumbling block in ensuring quality healthcare in the United States of America as huge chunks of the funds are dedicated to activities that add little value to the overall healthcare. Figure 1 below illustrates the USA’s administrative costs as compared to other developed nations and it shows the country’s costs at a whopping $752 compared to, say France at $37.
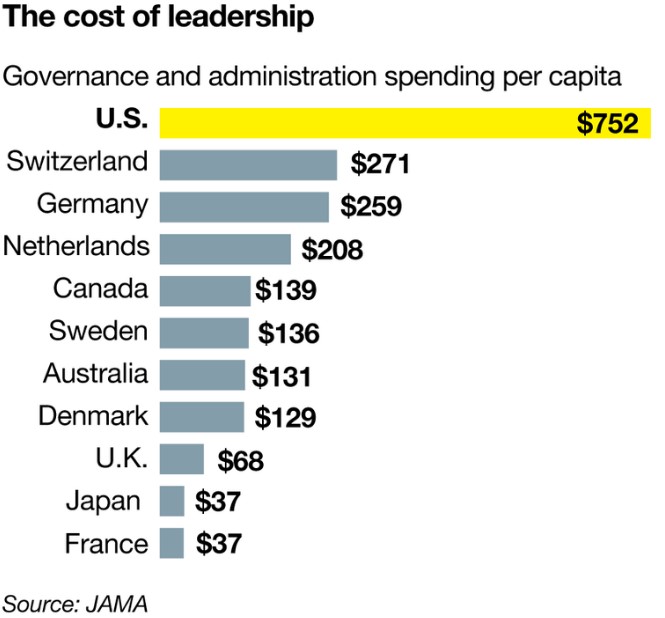
Figure 1: USA’s exorbitant administrative costs
The USA also pays medical practitioners more than other affluent nations, according to the JAMA study, and this is partly attributed to America’s obsession with maximizing revenue and profit orientation (Meyer, 2018) as part of the country’s capitalism philosophy. To this end, healthcare provision is more of a profit-making enterprise whose objective is to maximize revenue and in the end; the costs are bound to escalate in all aspects that include salaries for nurses and physicians as well as costs for services and procedures (ibid). The solution to this quandary might lie in the government setting overall spending thresholds as is the case in other developed nations as a way of curbing the steeper prices for drugs and medical costs for the processing of medical claims (Rapaport, 2018, p.3).
The USA is also characterized by inequalities in innovation, costs and outcomes that are region-specific as compared to other affluent countries (Rapaport, 2018) and the underperforming regions in terms of research and scientific innovation cause America as a whole to lag behind its peers in the quality of healthcare. In addition, America’s income distribution is skewed making some sections of the population very poor while others are very rich. The poor’s access to health and other social determinants of health, such as economic stability, education, social and community context, neighborhood and built environment (Health People 2020, 2019, p.1) are shoddy and this partly explains why life expectancy and infant mortality rates are higher in the United States of America than in other developed nations. For instance, the influx of undocumented immigrants into the country from countries such as Mexico and other Latin American countries has not only put a strain on the country’s health delivery system but also contributes to the low performance of the sector as the immigrants’ access to health is compromised due to the presence of social barriers to health (Health People 2020, 2019).
America’s incentive system does not result in improved quality of healthcare system since medical service providers and hospitals have received incentives for quite some time to make healthcare services and medications affordable through the Accountable Care Act and other programs but there is little evidence to suggest that the incentives resulted in improved performance (Ryan, Sutton, and Doran, 2014). The poor use of the incentives and the huge administrative costs dilute the impact of the incentives and in the end, the desired end results are not achieved.
In conclusion, the underachievement of the USA’s healthcare system as compared to other wealthy nations is paradoxical in the sense that the country spends more but the results are appalling. There is, therefore, a need for policies that promote a better quality of health by reducing costs of services, procedures and salaries for practitioners; improving the incentive system to ensure efficacy; while at the same time ensuring the availability of a vibrant universal health care insurance. Furthermore, America’s skewed income distribution calls for the government to address social determinants of health such as food and housing security as a way of boosting health outcomes and reducing costs.
References
Commonwealth Fund (2019). US spends more on health that other high income nations but has lower life expectance, worse health. Available at https://www.commonweatlhfund.org/https://www.commonwealthfund.org/press-release/2015/us-spends-more-health-care-other-high-utibncome-nations-has-lower-life-expectancy. Last accessed on 17 December 2019.
Health People 2020 (2019). Social determinants of health: Breaking down the barriers. HIMSS, 6 August 2019.
Johnson, K. (2018). Evaluating the Essentials of the U.S. Healthcare Essentials. Available at https://blogkjohnson.wordpress.com/2018/11/06/evaluating-the-essentials-of-the-u-s-healthcare-essentials/. Last accessed on 17 December 2019.
Meyer, H. (2018). Why does the U.S. spend so much more on healthcare? It’s the prices. Available at https://www.modernhealthcare.com/article/20180407/NEWS/180409939/why-does-the-u-s-spend-so-much-more-on-healthcare-it-s-the-prices. Last accessed on 18 December 2019.
Rapaport, L. (2018). U.S. health spending twice other countries’ with worse results. Reuters [online]. Available at https://www.reuters.com/article/us-health-spending/u-s-health-spending-twice-other-countries-with-worse-results-idUSKCN1GP2YN. Last accessed on 17 December 2019.
Ryan, A., Sutton, M. & Doran, T. (2014). Does winning a pay-for-performance bonus improve subsequent quality performance? Evidence from the Hospital Quality Incentive Demonstration. Health Services Research, 49(2), 568-587. doi:10.1111/1475-6773.12097.
Schuster, M.A.; McGlynn, E.A.; & Brook, R.H. (2005). How good is the quality of health care in the United States? National Center for Biotechnology Information. Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2690270/. Last accessed on 17 December 2019.
WHO (2018). Delivering quality health services: A global imperative for universal health coverage. Available at https://creativecommons.org/licenses/by-nc-sa/3.0/igo. Last accessed on 18 December 2019.
This is an example post, originally published as part of Blogging University. Enroll in one of our ten programs, and start your blog right.
You’re going to publish a post today. Don’t worry about how your blog looks. Don’t worry if you haven’t given it a name yet, or you’re feeling overwhelmed. Just click the “New Post” button, and tell us why you’re here.
Why do this?
The post can be short or long, a personal intro to your life or a bloggy mission statement, a manifesto for the future or a simple outline of your the types of things you hope to publish.
To help you get started, here are a few questions:
You’re not locked into any of this; one of the wonderful things about blogs is how they constantly evolve as we learn, grow, and interact with one another — but it’s good to know where and why you started, and articulating your goals may just give you a few other post ideas.
Can’t think how to get started? Just write the first thing that pops into your head. Anne Lamott, author of a book on writing we love, says that you need to give yourself permission to write a “crappy first draft”. Anne makes a great point — just start writing, and worry about editing it later.
When you’re ready to publish, give your post three to five tags that describe your blog’s focus — writing, photography, fiction, parenting, food, cars, movies, sports, whatever. These tags will help others who care about your topics find you in the Reader. Make sure one of the tags is “zerotohero,” so other new bloggers can find you, too.
